Clinical care costs rise without end because its core input, a clinician’s judgment, is delivered one patient at a time and cannot be sped up. Two economic ideas, Baumol’s cost disease and the Jevons paradox, point to one way to bend the cost curve: an AI that safely makes the routine clinical decision itself and escalates the rest to a clinician. Assistive tools speed the work around the decision and leave the cost where it is. A regulated system that makes the decision takes that work off the clinician’s hours, and because the supervision it provides is cheap, it expands care and frees clinicians rather than replacing them. RecovryAI is building this category, which it calls Prescribed AI, for post-surgical recovery; the device is investigational today and not authorized for commercial use.
Health care in the United States now costs 18 percent of everything the country produces, about 5.3 trillion dollars a year, and that share has climbed for half a century through every reform meant to bring it down.1 The cause is older and stranger than waste or fraud. Two economists, one who studied orchestras and one who studied coal, explain both why the cost keeps rising and how it finally falls. The way out is the same exit every other industry eventually found: a machine that takes over the core task, which in medicine means an AI that can make the routine clinical decision itself, built as a regulated medical device rather than the consumer “AI doctor” in the headlines. And the same move that bends the cost turns out to expand care and add capacity to a workforce that is running out of people.
A Law From the Concert Hall
The economists William Baumol and William Bowen found the law in the 1960s, and not in a hospital. They were studying orchestras. A Beethoven string quartet takes four musicians about forty minutes to play, the same as it did two centuries ago. You cannot play it faster, or with three musicians, and have it still be the piece. The work cannot be made more productive, because the work is the human effort itself.
Over those same two centuries, the musicians’ pay rose anyway, and by a lot. A skilled violinist can always leave for a job in a part of the economy that did get more productive, and better paid, so to keep her the orchestra has to match what she could earn elsewhere. Pay is set across the whole economy. Productivity is not. Any work that cannot be sped up still has to pay the going wage, so its cost climbs forever, with nothing to show for the climb. Economists call it Baumol’s cost disease. Baumol spent the rest of his life tracing it, and titled his last book, in 2012, “The Cost Disease: Why Computers Get Cheaper and Health Care Doesn’t.”
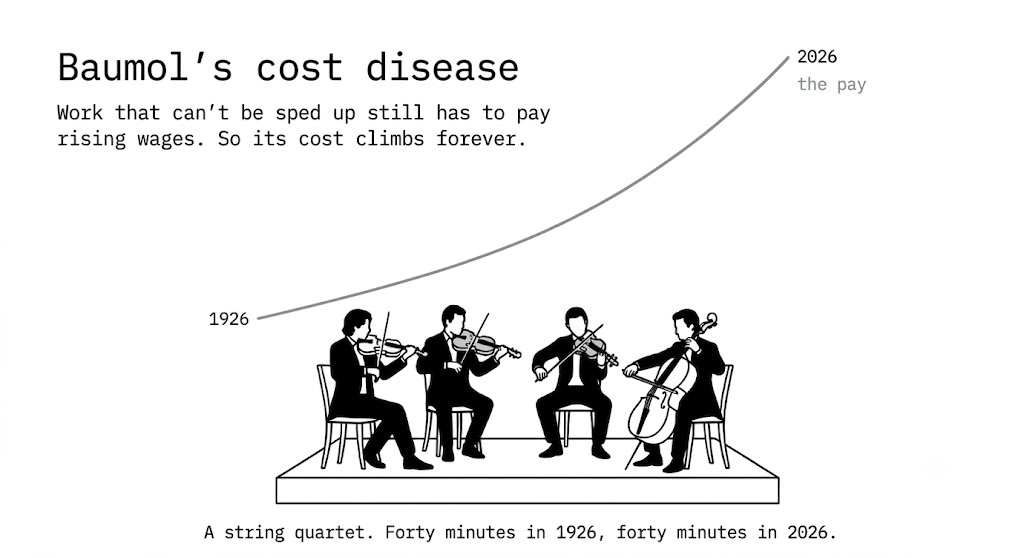
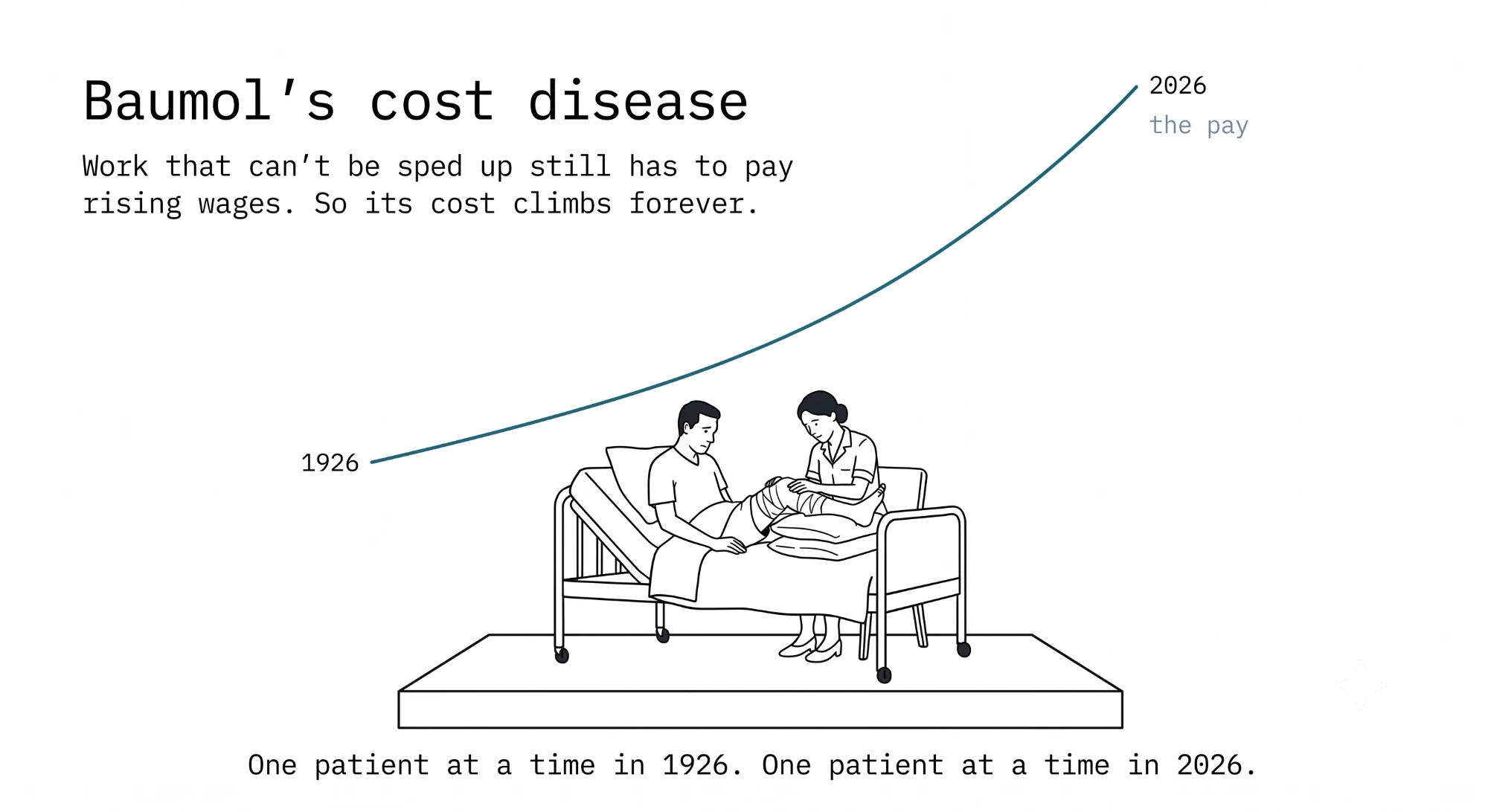
Clinical care has the disease for the same reason the quartet does. It runs on human time and judgment that resist being rushed. A careful look at a worried patient after surgery takes about as long as it always has, and hurrying it changes what it is. The rising bill reflects no error in how medicine is practiced. It is the price of work a machine has never been able to do.
Baumol’s cost disease has no cure in productivity gains alone. The only escape is a machine that performs the bounded clinical decision itself, moving the core task from human labor to silicon. Without that move, health care costs will rise with wages forever.
That is the mechanism. That is the trap, and it is the only exit.
The Only Exit Anyone Has Found
Some industries did escape the disease, and they all escaped it the same way. A machine took over the routine task itself. In 1900 about two in five American workers farmed; today a few percent do, and they grow far more food.2 The tractor and the combine did the plowing and the harvesting; a stronger horse or an extra farmhand would only have moved the same work around. But farms did not shrink, they expanded. More land got farmed, more crops grew, and the farmworkers who stayed moved into soil management, crop selection, and market decisions, the work machines could not do. The telephone network kept growing because automatic switching connected the calls, where no amount of hiring switchboard operators could have carried a century of growth. But the switching centers multiplied, and the operators moved into customer service, handling problems, and selling services. In every case the leap came from a machine doing the routine labor-intensive work, but the skilled decisions that only a human could make stayed with the person, and the sector expanded.
The test is simple, and health care is about to fail half of it and pass the other half. A wave of genuinely useful software has arrived in medicine. Ambient scribes write the clinical note from the conversation in the room and hand physicians back their evenings. Copilots summarize a sprawling chart in seconds. Smart inboxes triage the message queue. These tools are good, they are getting better fast, and any practice should use them. Every one of them makes the people around the clinical decision faster, but the decision itself still belongs to the clinician, made for one patient at a time. The work around the decision gets lighter. The labor that drives the cost is the decision, and it does not change, so the cost curve does not move.
The Jevons Paradox, and What the ATM Did for the Teller
The exit, then, is to let a machine make the routine clinical decision, the low-acuity slice that repeats, while the complex judgment stays with the clinician. The reasonable objection is that the routine work is the job, so automating the routine takes the job with it. The record points the other way.
Between the early 1980s and 2010, American banks installed about 400,000 automated teller machines. The obvious prediction was the end of the bank teller. Instead the number of tellers rose over those years, from about 500,000 to nearly 600,000.3 The ATM took over the routine task of handing out cash, which made a branch cheaper to run, so banks opened far more branches, and the tellers moved into the work a machine could not do: opening accounts, handling problems, and selling services. The routine task left human hands, and the people moved up to the rest of the job.
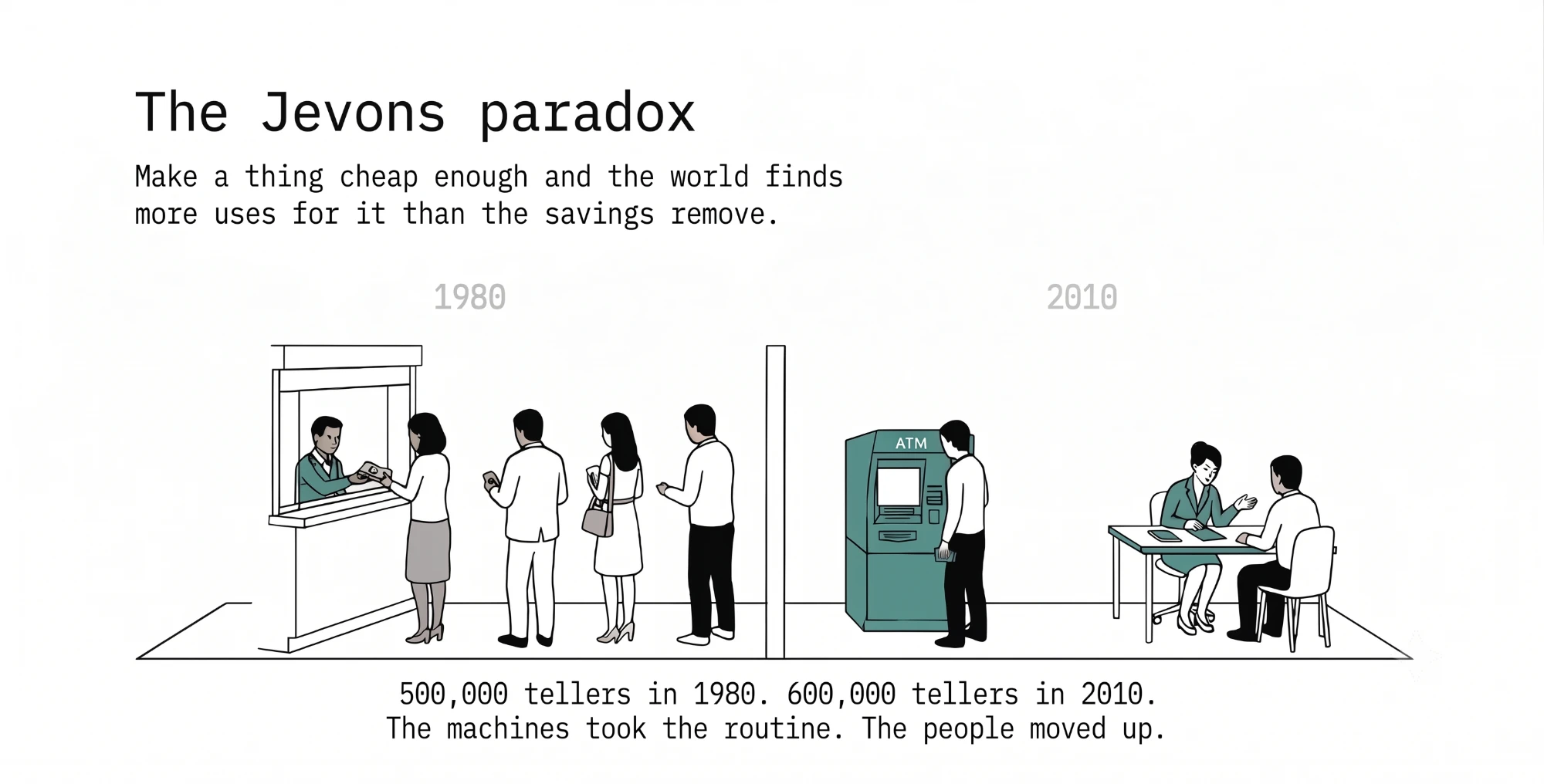
That outcome is not automatic, and it would be dishonest to sell it as inevitable. Automation has ended plenty of jobs for good. The teller pattern holds under one condition: a machine takes a routine task inside work that people want far more of, the lower cost expands the work, and the humans are pulled toward the parts a machine cannot do. Economists call this the Jevons paradox, after William Stanley Jevons, who found it in 1865 watching coal. When the steam engine grew efficient and burned less coal for the same job, Britain burned more coal, because cheap steam power was suddenly worth using everywhere. Make something cheap enough and the world finds far more uses for it than the savings ever remove.
Where It Applies, and Where to Start
Put the two together, the cost disease and the Jevons paradox, and you get the case for a new kind of tool that reaches across the whole health system. The thing that cannot be sped up is the same everywhere in medicine: a licensed human making a clinical judgment, one patient at a time. It is the primary care visit, the message between visits, the after-hours call, the chronic condition managed month by month, and the recovery watched at home. Wherever that judgment is the bottleneck, the cost disease is at work, and the exit is the one every other industry took: a machine that can make the bounded, routine part of the judgment itself, safely, and hand the rest to a person.
You cannot do that everywhere at once. RecovryAI has identified post-surgical recovery as that place. A recovery follows a known clinical script, the risk is concentrated in the first weeks, a missed problem shows up plainly as a readmission, and, as of this year, Medicare has begun paying hospitals to own the whole episode.4 It is the cleanest place to prove the idea and the first place it pays.
One Move, Two Results
In post-surgical recovery, most of what reaches a clinician is one question asked over and over: is what this patient feels part of normal healing, or the first sign of something wrong? After a knee or hip replacement it shows up as the expected pain, the swelling that is on schedule, the wound that looks worse than it is, and the medication and mobility questions that come up in nearly every recovery. A clinician answers each one, one patient at a time, limited by the hours in the day.
A system that can answer that question reliably, and prove that it answers reliably, can answer it for every patient at home at the same time, and send the case that is not routine to a person. We call it a Virtual Care Assistant. It is the tractor for the routine clinical decision, and it does two things from one move.
First, it performs the Baumol escape. It moves the routine clinical decision, the part of the clinical work that was locked to one clinician and one patient at a time, from a person to a machine. That slice of the work stops costing clinician-hours, so its cost stops rising with the wage. The curve bends for the same reason it bent when the tractor took the plow: the core task stopped being something only a human could do.
Second, most of a recovery goes unwatched today, checked by a phone call and a visit at two weeks while the riskiest days pass with no one looking. Because keeping a clinical eye on a recovery is now cheap, far more of it gets done: every patient watched through the first weeks, the patient who would have waited too long to call reached early, the rural patient followed where no local clinician had the hours. That is the Jevons expansion, filling a gap that was always there, and it grows two things at once, the reach of care and the room for nurses to spend their time on the patients who need them. There are not enough of those nurses: HRSA projects a 10 percent shortage of registered nurses by 2027, and 24 percent in rural areas.5 Capacity and cost move in the same direction, from the same tool. The payment system is shifting to reward exactly this, which is a story for the next issue.
The One Condition
There is a hard condition, and it is the reason this is difficult to build and safe to rely on once built. A system that makes a clinical decision on its own is standing in for a licensed clinician, making a call a trained and accountable person would otherwise make. It has to be held to the same standard as that person.
This is where the phrase “AI doctor” does real damage, because it blurs the line between a chatbot and a medical device. Consumer chatbots answering medical questions operate outside any regulatory framework, making them unauditable and unsafe. A regulated device, by contrast, is bounded in exactly what it will and will not decide, clinically validated through rigorous pivotal trials, and authorized by the FDA on the strength of that evidence, and fully auditable. Anyone can ship the first kind. Standing behind the second is the hard part, and it is the difference between a tool you can trust with a safe clinical decision and one you cannot.
This is the category we are building at RecovryAI. Prescribed AI is an FDA-regulated, patient-facing system that stands in for a licensed provider on a bounded, and growing, share of the clinical decision, inside the care path. Our Virtual Care Assistant is designed to shift the routine clinical decision from the licensed provider to the device, allowing the provider to focus on the complex judgment that requires human expertise.
The ATM Story in Recovery, 2036
Run the ATM story forward and you can see the shape of the claim. Picture it told from 2036. Health systems put machines to work on the recovery question, is this normal healing or the first sign of trouble, and the prediction was the end of the recovery nurse. Instead there were more of them. Automated recovery monitoring had become cheap, so health systems watched far more of them: every discharge followed daily instead of a phone call and a two-week visit, rural counties covered for the first time, and recoveries that once needed a skilled-nursing bed finished at home. The cheap automated recovery had become the norm, and the nurse moved up the way the teller did, from asking the routine question a hundred times a day to handling the five patients each morning the machine could not clear.
That is the story the pattern predicts. It is not the story yet. A pivotal study settles the safety question first. Whether the Jevons expansion actually happens in the care path, whether automated recovery monitoring truly frees nurses and expands care, that is the question the field will answer once the device is deployed at scale.
1. Centers for Medicare & Medicaid Services, National Health Expenditure Accounts. U.S. health spending reached 18.0 percent of GDP, about 5.3 trillion dollars, in 2024.
2. U.S. Census Bureau and U.S. Department of Agriculture historical data on farm employment as a share of the U.S. workforce.
3. James Bessen, Boston University School of Law, Learning by Doing (2015) and “Toil and Technology,” IMF Finance and Development (2015).
4. Centers for Medicare & Medicaid Services, Transforming Episode Accountability Model (TEAM), a mandatory bundled-payment model effective January 1, 2026 for selected hospitals, covering five surgical categories including lower-extremity joint replacement, with 30-day post-discharge accountability.
5. Health Resources and Services Administration, National Center for Health Workforce Analysis, registered nurse workforce projections (2025).